If your CPAP machine is sitting on the nightstand more than it's sitting on your face, you're not alone. Many adults with sleep apnea start treatment with good intentions, then run into actual problems nobody enjoys talking about. The mask feels confining. Air pressure feels awkward. Sleep still doesn't feel restful. You wake up tired and wonder what comes next.
That question often brings people into a dental sleep medicine office. Sleep apnea isn't only about snoring. It can also be about how your jaw, tongue, soft palate, and nasal airway work together while you sleep. When those structures narrow or collapse, breathing becomes harder. For some people, the right next step is an oral appliance. For others, a surgical consultation may make sense.
If you're in Walnut Creek and trying to understand sleep apnea treatment surgery without getting buried in medical jargon, a clear roadmap helps. You need to know when surgery is considered, what each procedure does, and how to tell whether a surgical path fits your anatomy, symptoms, and treatment history.
Searching for Sleep Apnea Treatment Beyond CPAP in Walnut Creek
A common story sounds like this. You were diagnosed with obstructive sleep apnea, you tried CPAP, and at first you hoped it would solve everything. Then real life took over. Maybe the mask bothered your skin, maybe the hose made sleep feel complicated, or maybe you were unable to keep it on through the night.

That frustration can feel especially discouraging because sleep apnea affects more than nighttime breathing. Patients often describe brain fog, morning headaches, irritability, dry mouth, and the constant sense that they never fully recharged. It can also strain relationships when snoring, restless sleep, or repeated awakenings affect a partner too.
Why many patients start by asking about alternatives
In dental sleep medicine, one of the most important things we do is slow the process down and ask better questions. Is the main problem CPAP comfort? Is nasal breathing limited? Does your jaw position leave less room for the tongue? Is your airway narrowing mostly at the soft palate, the tongue base, or several places at once?
Those details matter because surgery isn't one single treatment. It's a group of procedures designed to open or stabilize a specific part of the airway. Some people need a less invasive option first. Others need a broader evaluation because their sleep apnea isn't being driven by just one blockage.
If you'd like to understand the non-surgical side before thinking about surgery, our sleep apnea treatment options at our Walnut Creek office explain how dental sleep medicine can fit into the process.
The right plan starts with the reason your airway is closing, not with the most dramatic treatment on the menu.
Why a dentist may be part of this conversation
Many patients are surprised to learn that a dentist trained in sleep apnea care can play a central role in the decision process. That's because the mouth, jaw, tongue posture, bite, and airway shape all overlap. In some cases, an oral appliance can help move the lower jaw into a position that supports easier breathing during sleep. In other cases, that exam helps identify when a surgical referral is worth discussing.
At a local practice in Walnut Creek, this conversation should feel calm and practical. You shouldn't be pushed toward a one-size-fits-all answer. You should leave understanding your options and what each path is trying to fix.
Is Surgery the Right Next Step for Your Sleep Apnea
You may be at the point where the mask sits on the nightstand more than on your face. You wanted CPAP to work. You gave it time, adjusted settings, and tried to push through. Now you are wondering whether surgery is the next logical step or a step you might regret.
For many patients, surgery enters the conversation only after other treatments have been tried and the problem is still not well controlled. That does not make surgery the "strongest" treatment. It makes it a treatment that needs a precise target. Sleep apnea can come from different parts of the airway collapsing, much like a hallway that narrows at one door in one person and at several doors in another. A procedure only helps if it addresses the actual place, or places, where the airway is closing.
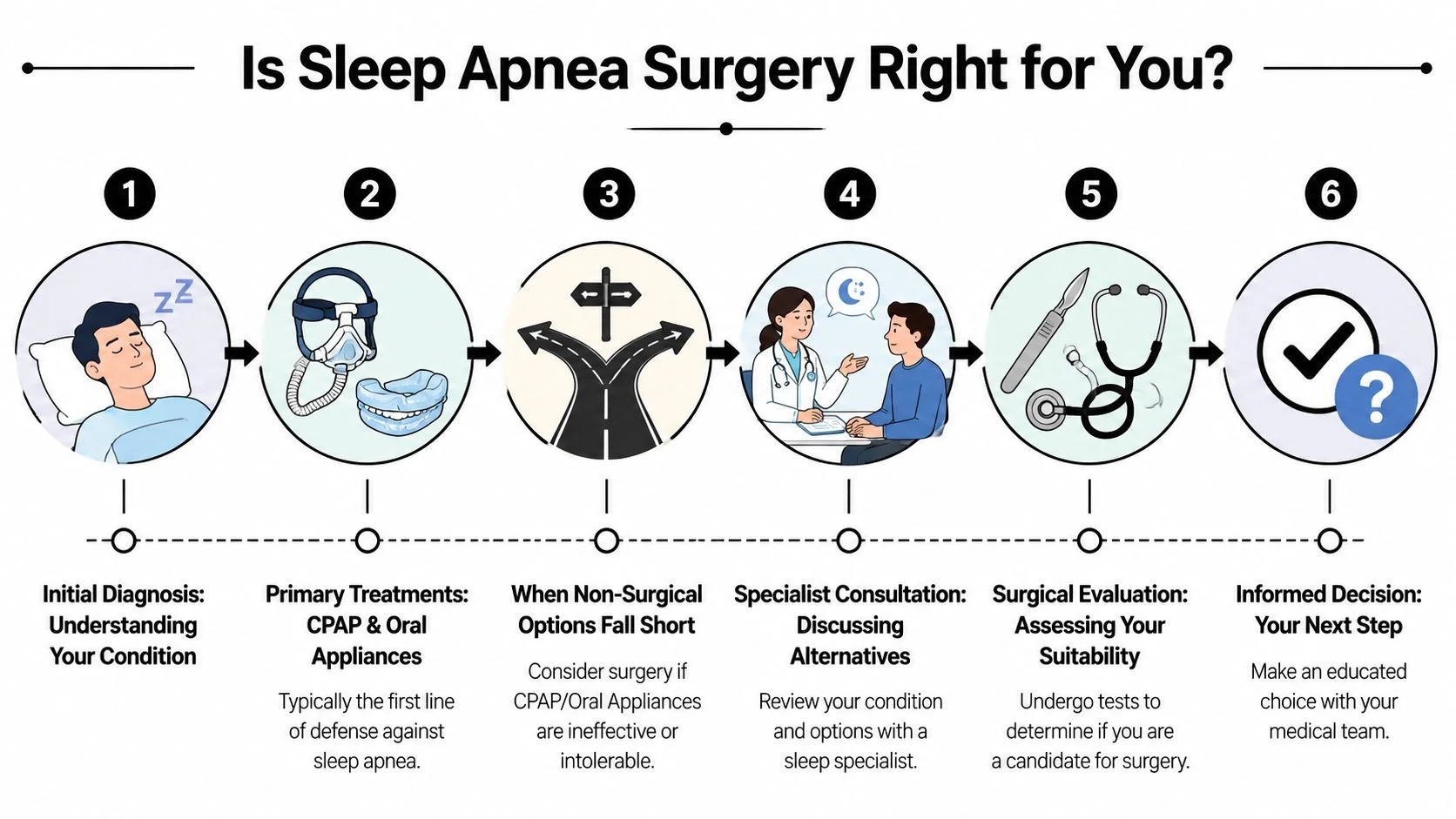
That is why the actual decision is rarely, "Do I want surgery?" A better question is, "What is causing my airway to collapse, and is there a procedure that matches that pattern?"
Signs that a surgical consultation may be reasonable
A surgical consultation may make sense if your treatment path has started to stall in one of these ways:
- You tried CPAP sincerely, but cannot tolerate it: The issue may be mask discomfort, pressure intolerance, claustrophobia, frequent awakenings, or the inability to keep it on long enough to help.
- Your anatomy suggests a structural blockage: Crowding at the soft palate, tongue base, nose, or jaw can make surgery worth discussing because the problem may be physical, not just positional.
- An oral appliance did not give enough improvement: Some airways respond well to jaw repositioning, while others still collapse in areas an appliance cannot correct well.
- Symptoms continue despite treatment efforts: Loud snoring, unrefreshing sleep, daytime fatigue, or witnessed breathing pauses can all signal that your current approach is not doing enough.
Some patients feel guilty at this stage, as if CPAP "should have worked" if they had tried harder. Please do not read it that way. Treatment failure often reflects a mismatch between the therapy and the airway, not a lack of effort.
The decision depends on fit, not intensity
Surgery is best understood as a customized repair plan. A palate procedure addresses one kind of narrowing. A jaw-based surgery addresses another. An implantable stimulation device is aimed at a different pattern altogether.
That is why a good consultation should slow the process down, not speed it up. You want someone to review your sleep study, your symptom history, what happened with CPAP or oral appliance therapy, and the physical features of your airway. In Walnut Creek, Dr. Schneider often helps patients work through this exact crossroads by clarifying whether the next step should be more non-surgical treatment, a referral for surgical evaluation, or a combination plan.
A calmer way to think about timing
You do not have to decide on surgery the moment it is mentioned. The next right step may be getting a clearer map.
For one patient, that map shows surgery is unnecessary because a better-fitted oral appliance or a different CPAP strategy may still help. For another, it confirms that months of frustration were pointing to a structural problem all along. Either result is useful. Clarity saves people from more guessing, more poor sleep, and more time spent trying treatments that do not match the problem.
A Patient Guide to Common Sleep Apnea Surgeries
A lot of patients reach this point after the same frustrating pattern. CPAP was prescribed, they tried to make it work, and they still wake up tired or feel like the machine never solved the underlying problem. At that stage, surgery can sound either too extreme or too vague.
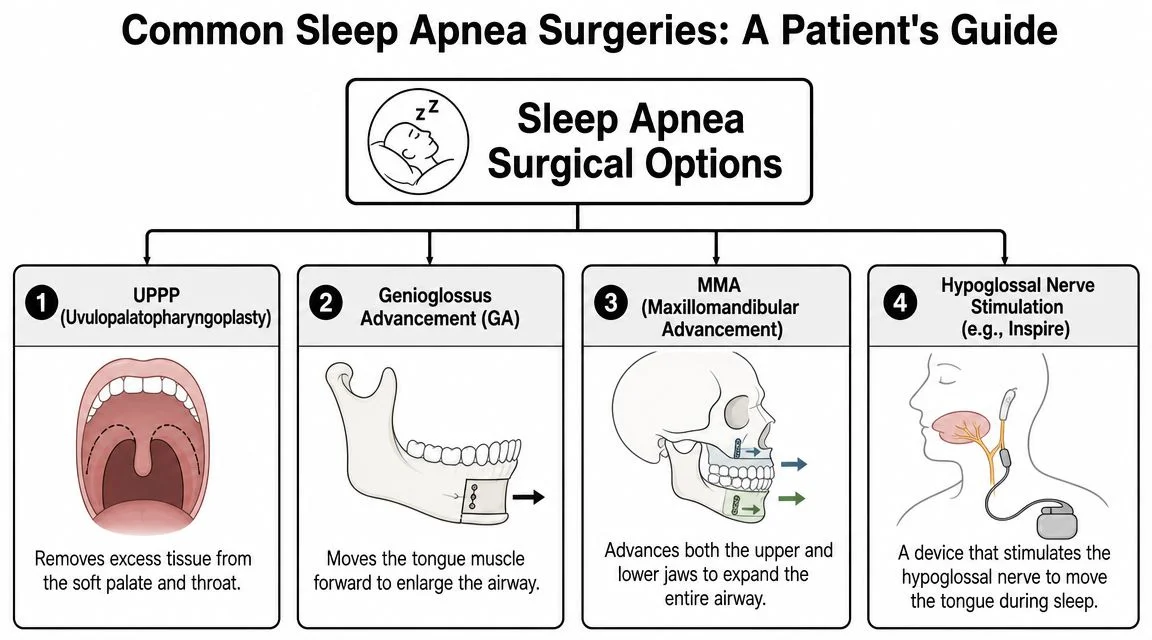
It helps to start with a simple idea. Sleep apnea surgery is not one operation. It is a group of procedures aimed at different parts of the airway, much like fixing a house with more than one narrow doorway. The nose can limit airflow. The soft palate can collapse backward. The tongue base can crowd the throat. Jaw position can leave too little room for the airway to stay open during sleep.
Soft palate and throat procedures
One of the best-known operations is UPPP, short for uvulopalatopharyngoplasty. In plain language, it removes or reshapes tissue in the soft palate and throat to create more breathing room. If the main bottleneck is at the back of the mouth, this type of procedure is meant to widen that area.
Tonsil removal may also be part of treatment. Large tonsils can physically crowd the throat, especially during sleep when muscle tone relaxes. For the right patient, removing them is a structural treatment, not a cosmetic one.
Nasal surgery and why it still matters
Nasal surgery is often misunderstood because patients sometimes hear two messages that seem to conflict. One is that nasal surgery alone usually does not fully resolve obstructive sleep apnea. The other is that it can still make a meaningful difference.
Both can be true.
Procedures that straighten a deviated septum or reduce enlarged nasal tissues can improve airflow through the nose. That may lower resistance, make nighttime breathing feel easier, and help some patients tolerate CPAP or other therapies better. In the decision-making process, that matters because a surgical plan is sometimes about improving the whole treatment path, not just checking off a cure.
Here is a short visual overview before we go further:
Tongue-focused procedures
For some patients, the main problem sits lower in the airway, behind the tongue. During sleep, the tongue can drift backward and narrow the space where air needs to pass. A palate procedure will not fully address that pattern if the tongue base is the larger issue.
A common example is genioglossus advancement. The name sounds technical, but the concept is straightforward. One of the main tongue muscles attaches to the lower jaw. By moving that attachment forward, the tongue gets better support and is less likely to collapse into the airway during sleep.
Why some patients need more than one approach
Many people do not have a single blockage. They have a combination of narrowing in the nose, palate, and tongue region. That is why two patients can both say they had sleep apnea surgery and mean very different things.
A mixed airway problem often needs a mixed plan. That may mean surgery plus CPAP, surgery plus an oral appliance, or more than one surgical approach chosen for different levels of the airway.
A quick online search can be confusing because it tends to lump very different procedures into one category. The better question is not, "Which surgery is best?" It is, "Where is your airway collapsing, and which treatment matches that pattern?" In Walnut Creek, that is where Dr. Schneider helps many patients slow the process down, sort through the options, and decide whether a surgical consultation makes sense as the next step after CPAP frustration.
Advanced Surgical Treatments for Severe Sleep Apnea
When sleep apnea is more complex, two options tend to come up often in serious treatment conversations. One is a structural jaw procedure called maxillomandibular advancement, or MMA. The other is hypoglossal nerve stimulation, an implant-based treatment designed for selected patients who cannot tolerate CPAP.
Maxillomandibular advancement
MMA is widely considered the strongest anatomic operation for obstructive sleep apnea because it moves both jaws forward and enlarges the airway behind the palate and behind the tongue. That matters because many patients don't have just one narrow spot. They have collapse at multiple levels.
A review available through PMC on surgical approaches for obstructive sleep apnea reports 86% to 90% surgical success and a 43% cure rate for MMA, using common endpoints of an AHI reduction by 50% plus postoperative AHI under 20 for success and AHI under 5 for cure. In that reviewed literature, MMA was the highest-efficacy option and was described as comparable in effectiveness to nasal CPAP in some studies.
Those numbers are encouraging, but they're not a promise for every patient. MMA is a major structural surgery. It tends to be considered when jaw position is a big part of the airway problem, especially when simpler treatments haven't delivered enough relief.
Hypoglossal nerve stimulation
Hypoglossal nerve stimulation is often described in patient-friendly terms as a pacemaker-like treatment for the tongue. The basic idea is that the device stimulates the nerve that helps control tongue movement so the tongue is less likely to collapse backward during sleep.
A recent Mayo Clinic professional update on obstructive sleep apnea surgery options describes a newly FDA-approved bilateral hypoglossal nerve stimulation device in August 2025 and outlines candidacy details that include age 22+, AHI 15 to 60, BMI up to 35, and CPAP intolerance. The same update notes practical differences from earlier systems, including a single small chin incision, external activation hardware, and no implanted battery changes every 8 to 10 years.
Why candidacy can feel confusing
Patients often hear about implantable options and assume "less invasive" means "right for anyone who dislikes CPAP." It doesn't work that way. Device-based treatment still requires surgery, follow-up, and meeting specific criteria. Some patients won't qualify because their airway collapse pattern doesn't fit what the device is designed to treat. Others may be excluded by sleep study findings or body habitus.
A simple way to think about the difference is this:
| Treatment | Main target | Best fit |
|---|---|---|
| MMA | Skeletal airway limitation | Patients whose jaw structure contributes to airway collapse |
| Hypoglossal nerve stimulation | Tongue-related collapse in selected candidates | Adults who meet device criteria and cannot tolerate CPAP |
Neither option is "better" in the abstract. Each solves a different problem.
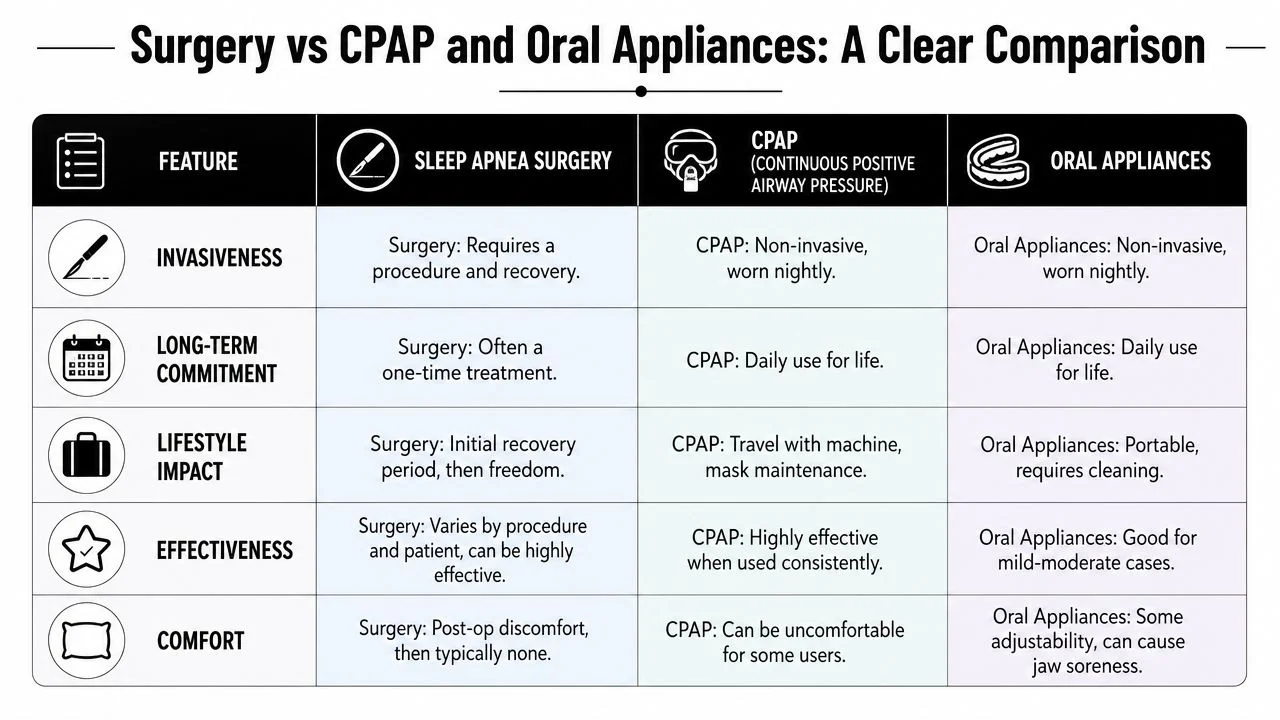
Surgery vs CPAP and Oral Appliances A Clear Comparison
The most useful comparison isn't which treatment sounds more advanced. It's which treatment you can use and which treatment matches your airway.
How the options differ in daily life
CPAP is highly effective when used consistently, but some people struggle with the nightly routine. The machine, mask, tubing, air pressure, cleaning, and travel logistics all matter. For patients who adapt well, it can work very well. For patients who don't, the effectiveness on paper doesn't always translate into real sleep.
Oral appliances are different. They are worn in the mouth during sleep and are often easier to travel with and easier to accept than CPAP. They can be especially useful when jaw positioning helps support the airway. At a dental office such as William M. Schneider, DDS, oral appliance therapy is one of the non-surgical options that may be discussed before a surgical path is considered.
Surgery changes the equation because it doesn't depend on putting something on every night. But that benefit comes with tradeoffs. Surgery involves recovery, risk, and a need for careful diagnosis so the procedure addresses the right obstruction site.
A side-by-side way to think about it
| Question | Surgery | CPAP | Oral appliance |
|---|---|---|---|
| What does it require each night | Usually nothing after healing | Mask and machine use | Appliance wear |
| Is it invasive | Yes | No | No |
| Can comfort affect success | Mostly during recovery | Yes, often | Yes, sometimes |
| Does anatomy matter | A great deal | Less for basic use | A great deal |
Which patients tend to lean toward each route
The key issue is patient fit. A discussion of patient selection and tradeoffs in sleep apnea surgery emphasizes that the choice depends heavily on anatomy, apnea severity, and the patient's ability to tolerate non-surgical therapies.
If CPAP works and you can use it, surgery may not be your best next step. If CPAP fails and your anatomy points to a correctable blockage, surgery may become much more reasonable.
This is why the decision shouldn't be framed as "surgery versus CPAP" in a competitive sense. For some patients, CPAP remains the right answer. For others, an oral appliance is the better fit. For others still, surgery becomes the clearest route because nightly adherence has become the main barrier.
Your Surgical Evaluation with Dr Schneider in Walnut Creek
A surgical evaluation should feel less like a sales conversation and more like a careful sorting process. When you come in with sleep apnea concerns, the first priority is understanding what you've already tried, how you've felt with those treatments, and what your sleep study and airway exam suggest about the source of the problem.
What your first visit may include
You can expect a detailed review of symptoms, previous diagnosis, and current treatment history. If you've used CPAP, the conversation often includes what made it hard to tolerate. If you've tried an oral appliance or another approach, that matters too.
The exam may also include evaluation of your bite, jaw position, tongue space, and oral structures that could influence airway behavior during sleep. Dental imaging can help support that review when needed. If you'd like to learn more about care pathways, our sleep apnea treatment center near Walnut Creek offers more information about what this type of evaluation can involve.
Why personalization matters
Two patients can look similar on the surface and need completely different recommendations. One person may be a good candidate for an oral appliance because the lower jaw can be repositioned in a useful way. Another may need referral for a surgical opinion because the airway appears constrained by palate tissue, tongue collapse, jaw structure, or a combination of those factors.
That doesn't mean every patient needs surgery. It means your treatment plan should be built around the reason your airway is narrowing.
A good consultation leaves you with a decision path. It shouldn't leave you guessing which specialist to call next or whether your anatomy was even considered.
Coordinating care when surgery enters the picture
If surgery seems relevant, the dental role often includes identifying the likely pattern, documenting what has or hasn't worked, and helping coordinate with the appropriate medical or surgical specialists. That collaborative approach is especially helpful when a patient may benefit from combined care rather than a single intervention.
For many Walnut Creek patients, the most reassuring part of the visit is hearing that they still have options. CPAP trouble doesn't mean treatment has failed. It means the next decision deserves more precision.
Schedule Your Sleep Apnea Consultation Today
If you're exhausted, frustrated, and unsure whether to keep struggling with CPAP or look into sleep apnea treatment surgery, a consultation can give you a clearer answer. You don't need to commit to surgery just to ask whether it makes sense. You only need a careful evaluation of your symptoms, anatomy, and treatment history.
That first step can help you sort out several important questions. Is your airway problem more likely to respond to an oral appliance? Is there a structural issue that deserves a surgical opinion? Are you dealing with more than one obstruction site? Those answers can save time and reduce the trial-and-error approach that leaves many people feeling stuck.
Patients in Walnut Creek and nearby East Bay communities often want practical guidance, not pressure. That's the right instinct. A thoughtful sleep apnea evaluation should help you understand your options in plain language and move toward treatment with more confidence.
If you're ready to talk through your next step, scheduling a consultation is the simplest place to begin.
If you're looking for compassionate guidance from William M. Schneider, DDS, schedule a consultation to discuss sleep apnea symptoms, CPAP difficulties, oral appliance therapy, and whether a surgical referral may be appropriate for your airway and treatment goals.